



Malposition of Right Atrial Lead of Permanent Pacemaker
- Kevin M. Rice, MD

- Nov 1, 2015
- 3 min read
Updated: Jul 26, 2021
Frequent palpitations and SOB • Xray of the Week
This patient complained of frequent palpitations and shortness of breath. Chest x-ray was performed, and subsequent device examination revealed inability to reliably depolarize the right atrium.

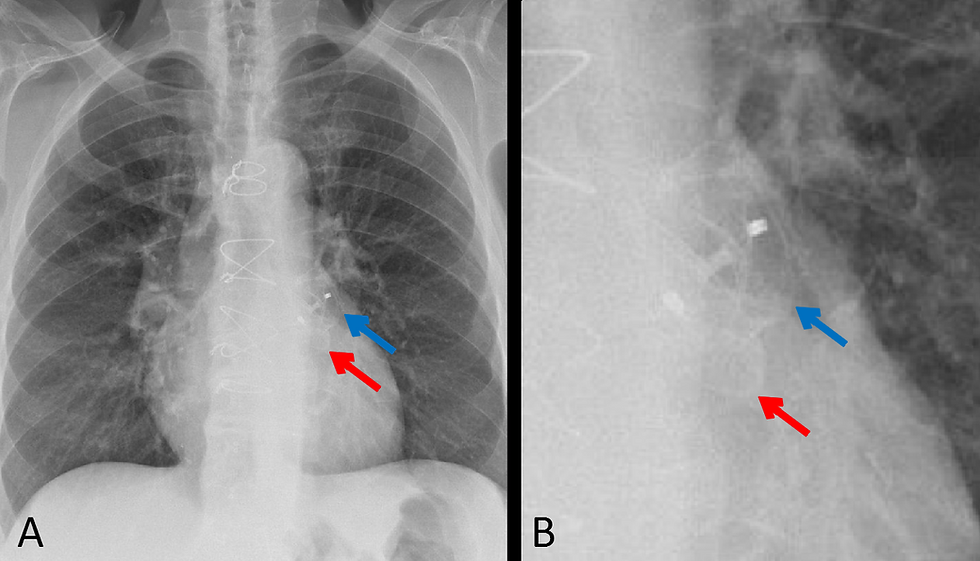
Fig. 1 RA lead (red arrow) of dual chamber pacemaker shows a slight curve on the initial post- placement image, and a straight vertical course on the 30 day image. The right ventricular (RV) lead is normally positioned at the RV apex (blue arrow). Images courtesy of my friend and colleague Marcelo Spector, MD.
In this case, the lead is floating freely in atrium, resulting in the inability to reliably depolarize the right atrium. This is probably due to placement with not enough "slack" in the lead to allow for motion during inspiration and standing erect.

Fig. 2 Dual lead pacemaker. RA lead (red arrow) of dual chamber pacemaker shows a normal "J" curve with the tip in the right atrial appendage. The right ventricular (RV) lead (blue arrow) is normally positioned at the RV apex.

Fig 3A. ICD–biventricular pacemaker combination. Frontal view. The shock coils of the ICD lead appear as thickened metallic sections visualized in the superior vena cava (SVC) and RV (blue arrows). The RA lead (red arrow) demonstrates a J-shaped appearance and curves superiorly and anteriorly with the tip in the right atrial appendage. The left ventricular (LV) lead is placed through the coronary sinus into a cardiac vein, usually along the lateral or posterior free wall of the LV (yellow arrow). The LV lead courses inferiorly and laterally on the frontal radiograph and posteriorly on the lateral view.

Fig 3B. ICD–biventricular pacemaker combination. Lateral view. The shock coils of the ICD lead appear as thickened metallic sections visualized in the superior vena cava (SVC) and RV (blue arrows). The RA lead (red arrow) demonstrates a J-shaped appearance and curves superiorly and anteriorly with the tip in the right atrial appendage. The left ventricular (LV) lead is placed through the coronary sinus into a cardiac vein, usually along the lateral or posterior free wall of the LV (yellow arrow). The LV lead courses inferiorly and laterally on the frontal radiograph and posteriorly on the lateral view.

Fig 4. ICD–biventricular pacemaker combination. Frontal view on another patient. The shock coils of the ICD lead appear as thickened metallic sections visualized in the superior vena cava (SVC) and RV (blue arrows). The RA lead (red arrow) demonstrates a J-shaped appearance and curves superiorly and laterally with the tip in the right atrial appendage. The left ventricular (LV) lead is placed through the coronary sinus into a cardiac vein, along the lateral or posterior free wall of the LV (yellow arrow). The LV lead courses inferiorly and laterally on this frontal radiograph
References:
1. Aguilera, AL MD, et al. Radiography of Cardiac Conduction Devices: A Comprehensive Review. RadioGraphics 2011; 31:1669–1682
2. Sigakis CJG, Mathai SK, et. al. Radiographic Review of Current Therapeutic and Monitoring Devices in the Chest. RadioGraphics 2018; 38:1027–1045
3. Brixey AG, Fuss C. Innovative Cardiac Devices on Chest Imaging An Update. J Thorac Imaging 2017;32:343–357
4. Costelloe, CM, MD, et al. Radiography of Pacemakers and Implantable Cardioverter Defibrillators. AJR 2012; 199:1252–1258
Related posts:

Kevin M. Rice, MD is the president of Global Radiology CME
Dr. Rice serves as the Medical Director of the Radiology Department of Valley Presbyterian Hospital in Los Angeles, California and is a radiologist with Renaissance Imaging Medical Associates. Dr. Rice has made several media appearances as part of his ongoing commitment to public education. Dr. Rice's passion for state of the art radiology and teaching includes acting as a guest lecturer at UCLA. In 2015, Dr. Rice launched Global Radiology CME to provide innovative radiology education at exciting international destinations, with the world's foremost authorities in their field.
Follow Dr. Rice on Twitter @KevinRiceMD













Comments